8 thoughts on “Making MORE THINGS HAPPEN with Jim DuCanto (with a bit of help from Cliff Reid & friends)”
Am I being dense?
Why not iGel – AmbuAscope with ETT preloaded – then intubate thro iGel?
Or AirQII?
Saves cutting the bronchoscope and risk of misplacement as remove LMA/place ETT
thanks Tim!
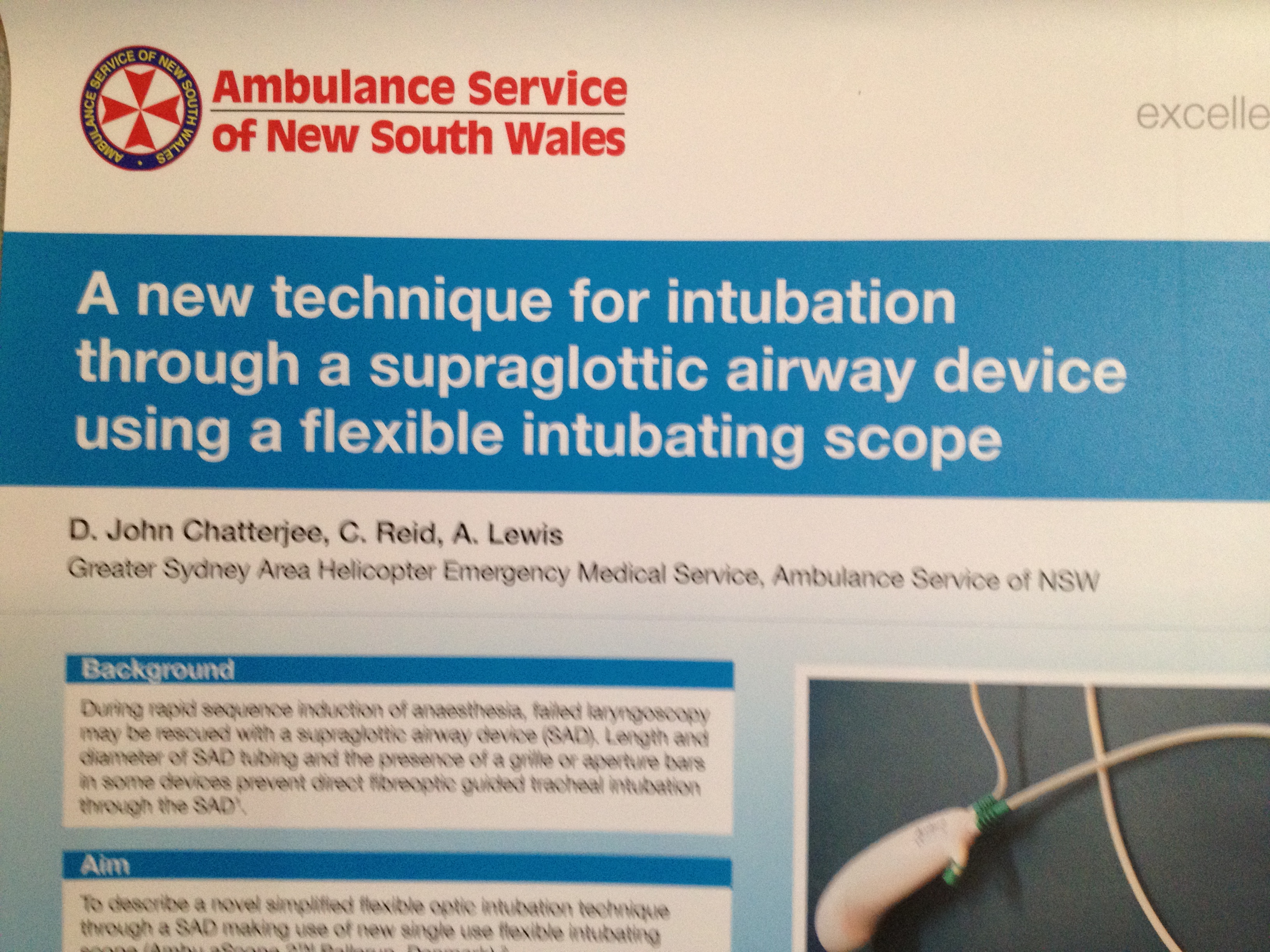
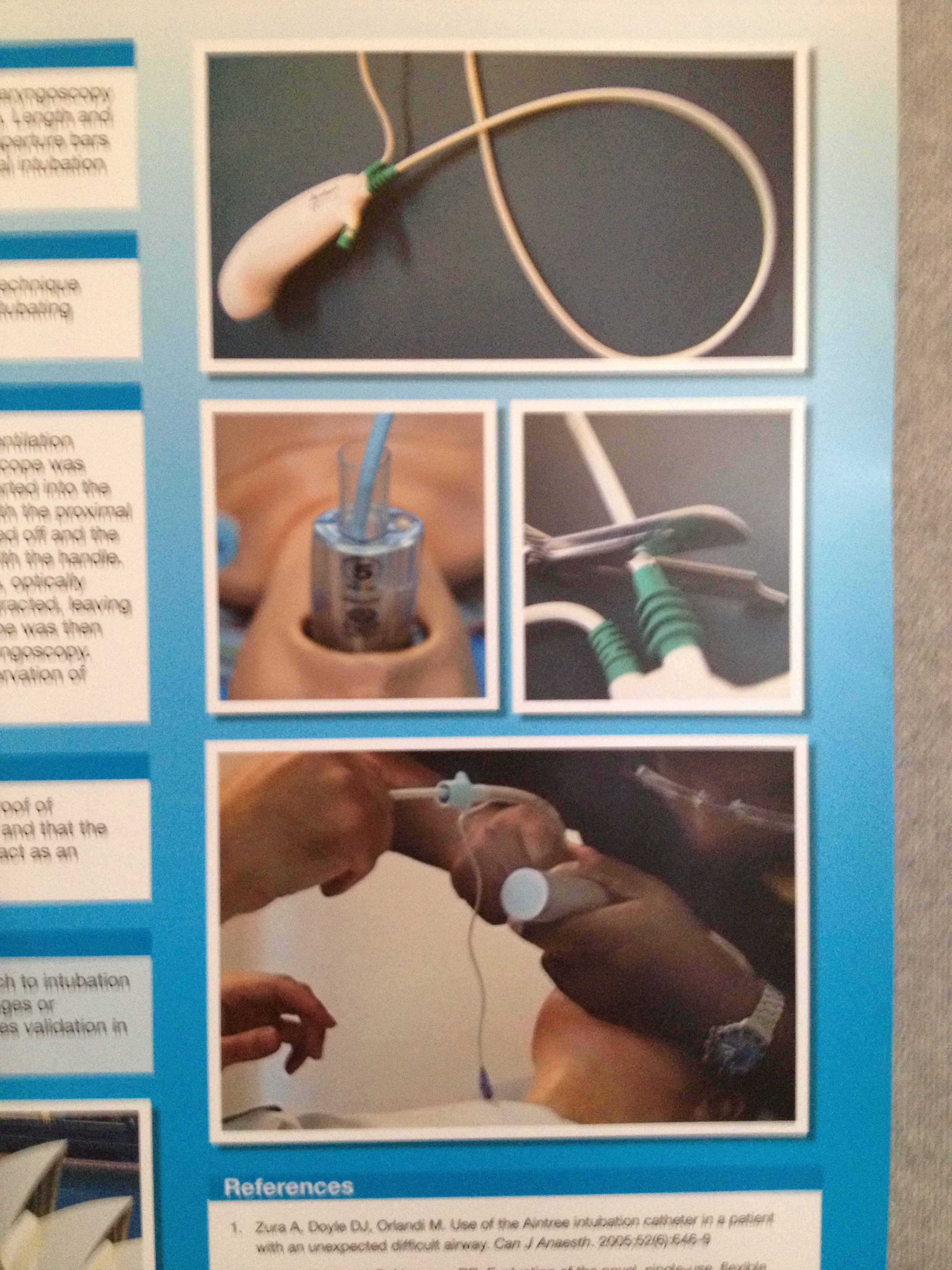
If you look at the images of the poster presentation, CLiff’s team describe exactly that. They use the iGel.
I imagine Jim did not have an iGel available or was just wanting to test if similar technique worked via a LMA SUpreme.
RFDS QLD carries the LMA Supreme and Fastrach ILMA so its nice to know that if we added an Ambu Ascope we have that option of tubing with it even via the Supreme.
its true that one potential pitfall of this technique using a SGA that you have to remove to railroad the ETT, is dislodging the scope shaft from the trachea and now you cant reuse it as you have just cut it!
Well—I wanted to reproduce what Cliff had described, and these were sales reps for the LMA Supreme. I do have a few iGels, and keep one for simulation. Through the iGel it’s easy–I wanted to see if it would work through the LMA Supreme. What I need to communicate is that if the Supreme is overinflated, the mask crunches in on the channel that the scope traverses. Almost exclusively, I utilize the Air-Q SGA for my elective cases (and utilize it to intubate the recognized and unrecognized difficult airways).
The pitfall that Minh points out can be obviated by placing the scope REAL DEEP, and then cutting the tracheal tube at 26-28 cm (reducing its length and dead space).
The simulation I performed was for my own curiosity, and of course, so I could “re-run the tape” and get that instant replay. That’s how I learn best.
Yes, I wasn’t being clear – why CUT it? I practiced with the Ambu a year ago on their propietary LMA, but don;t recall a need to cut the scope…
Can;t see why need to, but I must be missing something obvious here – why are you cutting it?
Got the Ambu guys coming over to KI later in year, as they do both the disposable scope and the KingVision now…can;t wait to pull ut my trauma shears and cut their demo model
I;ll blame it on Cliff….
well for the LMA Supreme you cant railroad an ETT over the Ascope..Supreme doesnt have the room to allow to do that.
as for iGel…I reckon you could do it but it would be a tight fit and you would need a smaller ETT. Cliff’s way you can exchange for a larger ETT I imagine and its smoother ETT passage.
Makes sense Minh…but I may stick with AirQ-2 / CookGas …many ways to skin the cat obviously.
I hear there is a new one that goes through an Aintree…bougie, then Scope/ETT
Need to practice on elective lists to keep hand in. Prob not good for soiled airway…but for the obese/predicted diff airway who needs intubation for transfer, this combo is very useful
Use the AmbuAScope with an cook Air Q, works great and no need to cut it to remove the AirQ saved the day with a 450lbs (204 Kg) plus pt. recently, but love this with the IGel, brilliant!
We wouldn’t cut it if intubating through an iGel, because everything fits (ETT 3 ‘sizes’ above iGel, eg. iGel size 4 will tolerate 7.0 mm ID ETT).
The cut scope idea was for an SGA with aperture bars or some obstruction to direct ETT passage through it.

Am I being dense?
Why not iGel – AmbuAscope with ETT preloaded – then intubate thro iGel?
Or AirQII?
Saves cutting the bronchoscope and risk of misplacement as remove LMA/place ETT
thanks Tim!
If you look at the images of the poster presentation, CLiff’s team describe exactly that. They use the iGel.
I imagine Jim did not have an iGel available or was just wanting to test if similar technique worked via a LMA SUpreme.
RFDS QLD carries the LMA Supreme and Fastrach ILMA so its nice to know that if we added an Ambu Ascope we have that option of tubing with it even via the Supreme.
its true that one potential pitfall of this technique using a SGA that you have to remove to railroad the ETT, is dislodging the scope shaft from the trachea and now you cant reuse it as you have just cut it!
Well—I wanted to reproduce what Cliff had described, and these were sales reps for the LMA Supreme. I do have a few iGels, and keep one for simulation. Through the iGel it’s easy–I wanted to see if it would work through the LMA Supreme. What I need to communicate is that if the Supreme is overinflated, the mask crunches in on the channel that the scope traverses. Almost exclusively, I utilize the Air-Q SGA for my elective cases (and utilize it to intubate the recognized and unrecognized difficult airways).
The pitfall that Minh points out can be obviated by placing the scope REAL DEEP, and then cutting the tracheal tube at 26-28 cm (reducing its length and dead space).
The simulation I performed was for my own curiosity, and of course, so I could “re-run the tape” and get that instant replay. That’s how I learn best.
Yes, I wasn’t being clear – why CUT it? I practiced with the Ambu a year ago on their propietary LMA, but don;t recall a need to cut the scope…
Can;t see why need to, but I must be missing something obvious here – why are you cutting it?
Got the Ambu guys coming over to KI later in year, as they do both the disposable scope and the KingVision now…can;t wait to pull ut my trauma shears and cut their demo model
I;ll blame it on Cliff….
well for the LMA Supreme you cant railroad an ETT over the Ascope..Supreme doesnt have the room to allow to do that.
as for iGel…I reckon you could do it but it would be a tight fit and you would need a smaller ETT. Cliff’s way you can exchange for a larger ETT I imagine and its smoother ETT passage.
Makes sense Minh…but I may stick with AirQ-2 / CookGas …many ways to skin the cat obviously.
I hear there is a new one that goes through an Aintree…bougie, then Scope/ETT
Need to practice on elective lists to keep hand in. Prob not good for soiled airway…but for the obese/predicted diff airway who needs intubation for transfer, this combo is very useful
Use the AmbuAScope with an cook Air Q, works great and no need to cut it to remove the AirQ saved the day with a 450lbs (204 Kg) plus pt. recently, but love this with the IGel, brilliant!
We wouldn’t cut it if intubating through an iGel, because everything fits (ETT 3 ‘sizes’ above iGel, eg. iGel size 4 will tolerate 7.0 mm ID ETT).
The cut scope idea was for an SGA with aperture bars or some obstruction to direct ETT passage through it.
See http://nswhems.files.wordpress.com/2011/09/c-18-advanced-airway.pdf for our options
The technique shouldn’t be necessary with an aScope 3 which will fil an Aintree
http://www.ambu.com/visualisation/ascope_system/ambu_ascope_3_slim.aspx
Cliff