( image attribution Ballon ventilation Wikipedia)
Hi folks.
An incredible week for me recently! Caught up with my airway skills mentor Dr Richard Levitan
A bit more on the nose thing in an upcoming post…
During his workshop, Richard gave some great insights into oxygenation issues in emergency airway management. As you know he coined the term NODESAT, which is about using nasal cannula oxygenation in the perintubation phase of RSI.
My anaesthesia colleagues have always seemed amused/puzzled by the benefit of nasal oxygenation despite most of the research into its benefit coming from anaesthesia!
After the workshop I suddenly realised the reason why anaesthesia folks just dont seem to think there is a need for NODESAT? You ever wondered that too?
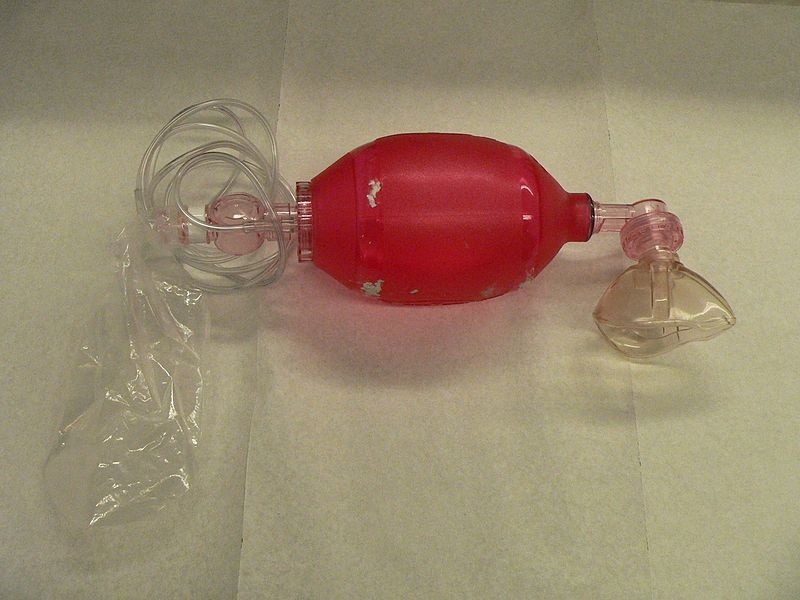
Well the secret is that the BVM ( Bag Valve Mask) manual resuscitator ( aka self inflating resuscitation bag mask) is a potential murder weapon…in fact more so than the laryngoscope!
(Editorial aside – if you have never heard of Scott Weingart’s seminal podcast series on Laryngoscope as a murder a weapon then check it out NOW WE WANT WEINGART)
WHAT!???
Well if you have been using the BVM to preoxygenate your emergency patients for RSI then it may come as a surprise to you that some BVM designs do not provide any more than FiO2 60% oxygen for spontaneously breathing patients! So much for assumed 100% oxygenation prior to RSI!
Which then answers the question why anaesthesia folks just dont get nasal cannula oxygenation.
Anaesthesia do NOT use BVM/self inflating manual resuscitators to oxygenate their patients prior to RSI. They use fresh gas flow circuits that deliver 100% oxygen to the patient mask. They preoxygenate their patients fully . They also use advanced gas monitoring with end tidal oxygen monitoring so they know when adequate denitrogenation of the lungs has occurred.
This is why they dont see much extra benefit from the nasal cannula oxygenation technique. For their purposes full preoxygenation gives most of the benefit.
This fact that some BVM designs do not deliver high oxygen concentrations to the spontaneous breathing patient has been known for some time with several studies showing this.
1. Inadequate preoxygenation during spontaneous ventilation with single patient use self-inflating resuscitation bags.
2. Efficacy of preoxygenation with tidal volume breathing. Comparison of breathing systems.
3. Oxygen delivery using self inflating resuscitation bags
4. Oxygen outflow delivered by manually operated self-inflating resuscitation bags in patients breathing spontaneously*
BOTTOM LINE : Know what your own BVM/manual resuscitation device system does in terms of oxygen delivery performance in spontaneously breathing patients as well as with manual ventilation!
If you are going to use it to preoxygenate Dr Levitan ( and now I !!) suggest adding in nasal cannula oxygenation technique to improve oxygen delivery !

{kind=link}
the first step, after the decision has been made to intubate, is to place a nasal cannula and turn that sucker up. whatever you do after the decision to intubate is done more safely with high flow oxygen via nasal cannula.
Click to access edictv13_screen.pdf
The failure of some BVMs to deliver 100% O2 has been revelatory for me too. There is potential for these devices to deliver little more FiO2 than would be achieved with 2Lt/min via nasal prongs!
I think the reason anaesthetists don’t use NODESAT, however, is simply that many don’t know about it. They still don’t use it even in out of theatre settings such as ECT, recovery or when in ED/ICU.
Certainly there is still significant benefit to be gained from NODESAT even when PreOx with 100% is undertaken as ApOx during laryngoscopy attempts will continue to deliver O2 to the alveoli providing the airway is patent (which it usually will be during larygoscopy) & there is an ongoing O2 source. ApOx should in fact be MORE effective the higher the FiO2 used for PreOx due to the higher O2 conc achieved in the respiratory tree. .
Thus nasal oxygen during airway management does much more than simply supplement the FiO2 of some poorly performing BVM devices and should not be viewed as an alternative to using high FiO2 delivering devices. Rather it is an adjunct which works synergistically with high FiO2 for PreOx. As such clinicians working in theatre should not omit NODESAT because they can deliver high FiO2 via their anaesthetic circuit, nor should clinicians outside theatre (incl anaesthetists) neglect to use a device capable of delivering a high FiO2 because they are using NODESAT. To maximise safe apnoea time you need a combination of PreOx, ReOx (vent between attempts when in Green Zone of Vortex), ApOx & MinDeOx (strategies to decrease O2 consumption such as minimising fasciculations with sux). We should be striving for excellence in all these aspects, not trading the benefits of one off against the other.
I completely Agree with Nick…I find NODESAT very useful even in OR especially for passive oxigenation during intubation and for selected surgical specialities such as Bariatric surgery….NODESAT guarantees a very prolonged time of Apnoea before Desaturation especially in pt. that usually desaturate very fast– personal experiences–
With a tight fitting mask seal and a BVM, the nasal cannula oxygen facilitates the preoxygenation process by increasing the overall flow during the inspiratory phase of ventilation, whether the patient is breathing spontaneously or not. Anytime you can create a BiPAP-type system (which is essentially what this is), it is worlds above older methods of preoxygenation.
If the patient is breathing spontaneously, a high flow nasal cannula will further add to the PEEP of the system (especially if a PEEP valve has been added to the system), reduce the work of breathing while using the BVM (by a “power” assist during the inspiratory phase) and so on.
Anesthesiologists are not as conscious about these details of preoxygenation as is inferred here–the greater majority of their cases do not challenge them to need to come up with innovative ways to cope with this problem–their equipment and methods have served them well. The cases in which preoxygenation is a definite challenge are rare in the operating room, and as a result, many anesthesiologist/specialists are unprepared to face these challenges, as they have not been challenged to bring BiPAP systems (or techniques, such as high flow nasal cannula) into the operating room. In a strange twist of fate, the Emergency Medicine community now has something to contribute to their Anesthesiology colleagues.
If your anesthesia colleagues seem dismissive on this topic, it is due to a lack of awareness and training on their part. What you guys are doing here is the right solution for one of the most dangerous problems in modern airway management.
I became more aware of the problem than many of my colleagues due to my “sub specialization” in handling the difficult airways in an 800+ bed tertiary care hospital. My department tends to send these cases my way due to my affinity and aptitude for them–most of my colleagues hate these cases, yet I flock to them. It was my introduction to and repeated use of a pre-hospital resuscitator that raised my awareness of this topic. In the operating room, I still use this pre-hospital resuscitator in preference to formal BiPAP systems–it’s more simple, easy to use and doesn’t need the care and feeding of an entire machine on wheels with ventilator tubing, alarms and such.
Without the availability of specialized equipment, the use of the nasal cannula at high flow is a missing link in emergency airway management.
BVMs are either fine (>90% fiO2) or they suck (close to room air). The dividing line is whether there is a one-way valve on the exhalation port. The ones we stock do not have one and therefore can’t be used without alteration for preox in spont breathing pts. You can test by cutting off the bag, occluding the cut portion and seeing if you can breath through BVM port.
Any bag can be fixed by simply adding a PEEP valve to it. Now you have your one-way valve back again and the bag will deliver >90% along with the ability to dial in PEEP.
Yep, gotta love the PEEP valve as an addition. Simple, low cost.
Bit like adding nasal cannulae.
Every little helps – not for “most” patients, but for those who need the edge – those who fall precipitously on the ‘oxy-hemo-coaster’
Hi Minh,
We use PEEP valves at the end of ours now and with high flow nasal cannulae in tandem, they’re actually fine for pre-ox needs in our xp.
Rahul
Just revisiting this. Shouldn’t PEEP valves be the de facto setting in ED/prehospital ,rather than available as an extra bit of kit to add on?
I know that I have been guilty of forgetting to add ’em – once I’ve placed a BMV on the patient and am ventilating, my mind is usually raising ahead to securing IV/IO access and intubation.
So – ensure the addition of a PEEP valve to the BMV device in your ED every shift…or as part of kit check in prehospital.
Sensible?