Evolution of inexpensive videolaryngoscopy: from concept to practice
Author:
Dr. John George Karippacheril,
Specialist Anaesthesiologist, Abu Dhabi,
Former Associate Professor of Anaesthesiology,
Manipal University, India.
Email: johngeorgedon@gmail.com
Twitter: @johngeorgedon
“Vision is the art of seeing what is invisible to others” — Jonathan Swift
Not many procedures in Medicine have received the attention and focus of medical practice, especially in critical care, as laryngoscopy. A secure airway serves as a lifeline to the critically ill, yet the process of securing it remains at times enigmatic, more of an art than a science. Inability to secure the airway or airway related critical incidents remains a cause of morbidity and mortality in hospitals globally. Not every physician or healthcare provider may have the training or the tools they need to achieve a high degree of competence.
But why is this procedure fraught with difficulties, with dangers lurking around the corner? Well, it depends on that corner which we need to look around! During laryngoscopy our visual axis is not aligned with the axis of the laryngeal structures. Our vision needs to traverse the near 90-degree turn of the base of the tongue, in order to view the larynx (Figure 1). Direct laryngoscopy attempts to flatten this corner, which can be a losing battle, when it’s a tight one. The laryngeal and visual axes may not be fully aligned, but what if we could virtually reach into the hypopharynx and look right down at the larynx? Surely, this would give the best view, thus the idea of videolaryngoscopy was conceived.
Figure 1
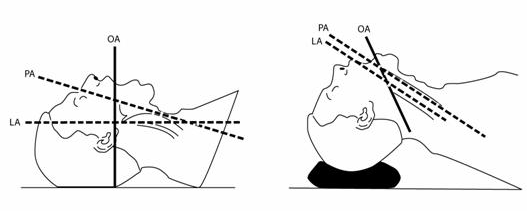
From Mendis D, Oates J. The Application of Airtraq (fibreoptic intubation device) to Otolaryngology. Online J Health Allied Scs. 2011;10(2):16; Accessed 2 April 2015 at URL: http://www.ojhas.org/issue38/2011-2-16.htm
Early commercial attempts at videolaryngoscopy in 2001 coupled complementary metal oxide semiconductors (CMOS) sensors with curved laryngoscope blades, a design concept prevalent even at present. The cost of these commercial devices run into thousands of dollars, often out of reach for resource constrained environments. In spite of the need of videolaryngoscopes for Pre-hospital, Emergency Medicine, Critical Care, and in Operating Rooms, adoption of videolaryngoscopes as a standard of care has been slow. The expensive initial cost of investment has played a major role.
Videolaryngoscopy can be done inexpensively. We could replicate the original concept by attaching a CMOS sensor to a conventional curved laryngoscope. The actual cost of manufacturing a 640×480 resolution sensor is only a few dollars. Several online retailers offer these sensors, in a waterproof casing with an universal serial bus (USB) interface, under the product name “USB endoscopic camera”. The product is in essence similar to a small sized webcam. Tomtop.com a Chinese retailer offers the devices for prices as low as 7$ for a 7mm diameter USB camera. These sensors have to be a hooked up to a color display for viewing. Most of us possess a mobile phone or laptop personal computer (PC) with a high-resolution color display and video processing that may be leveraged. For technical reasons, connection to a mobile phone hasn’t been as easy as in personal computers.
A common interface available for these sensors is through the universal serial bus (USB) port of the devices. PCs often have inbuilt drivers for these USB video class (UVC) devices that enables `plug and play’ functionality. Initial work on this concept, was done by the author and in a similar experiment by Minh Le Cong (Twitter handle @ketaminh) . In the author’s study on Inexpensive videolaryngoscopy using a PC, a waterproof USB camera (which costs less than 40$) was assembled onto a conventional Macintosh laryngoscope (Figure 2).
Figure 2
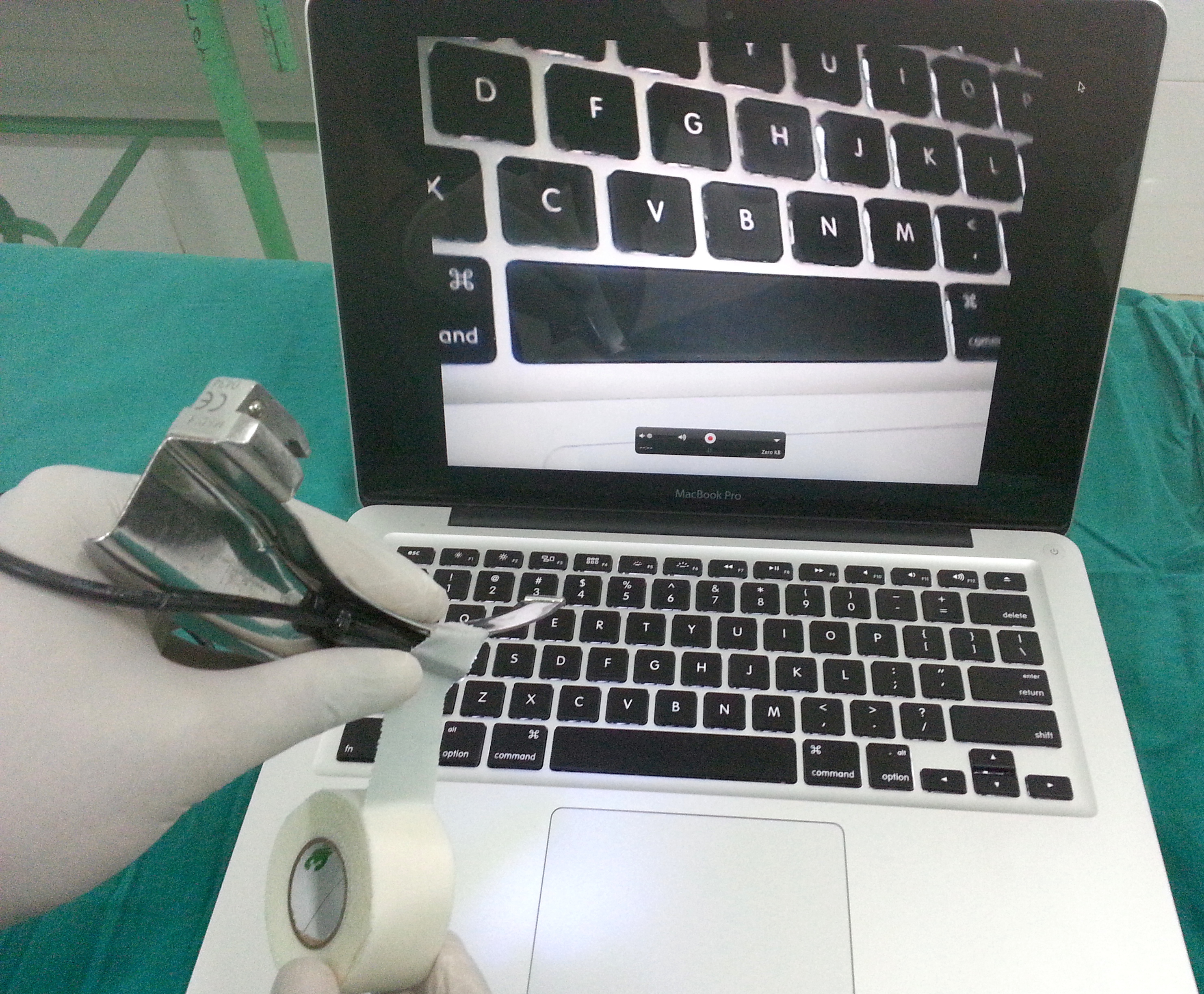
The camera was secured using a clean, adhesive tape (Durapore, 3M Inc., USA) approximately 40mm from the tip of the laryngoscope blade. This position was determined by trial and error, before the study, to give an optimal view of the laryngeal inlet. A position too close to the tip of the laryngoscope blade was associated with a view that was more zoomed in than necessary. Prior to fastening the camera, the device was rotated to visually orient the real-time image on the PC screen upright, using text on a keyboard (Figure 2). The waterproof device was disinfected after use by washing it with soap, water and wiping down with surgical spirit. Initial trials were done on manikins followed by a limited study, after approval, in a University teaching hospital. Successful laryngoscopy and intubation could be done in all patients with no adverse events, even in those with predictors of difficult laryngoscopy. High quality videos of laryngoscopy could be recorded in all patients using Windows (using webcam software), Mac OS X (using QuickTime Player) and Linux (using UVC viewer) operating systems.
The next obvious area of research would then be the ubiquitous mobile technology. However, with mobile phones or tablets, not all devices have an USB interface. Those that do have USB may not have drivers for UVC devices in their operating system kernel. The Android operating system (OS) for mobiles from version 3.1 and higher supports USB host on-the-go (OTG), that can load these kernel drivers on demand. USB devices can then be connected to the micro-USB port of these mobile devices using an OTG cable (a feature not supported in Apple iOS devices).
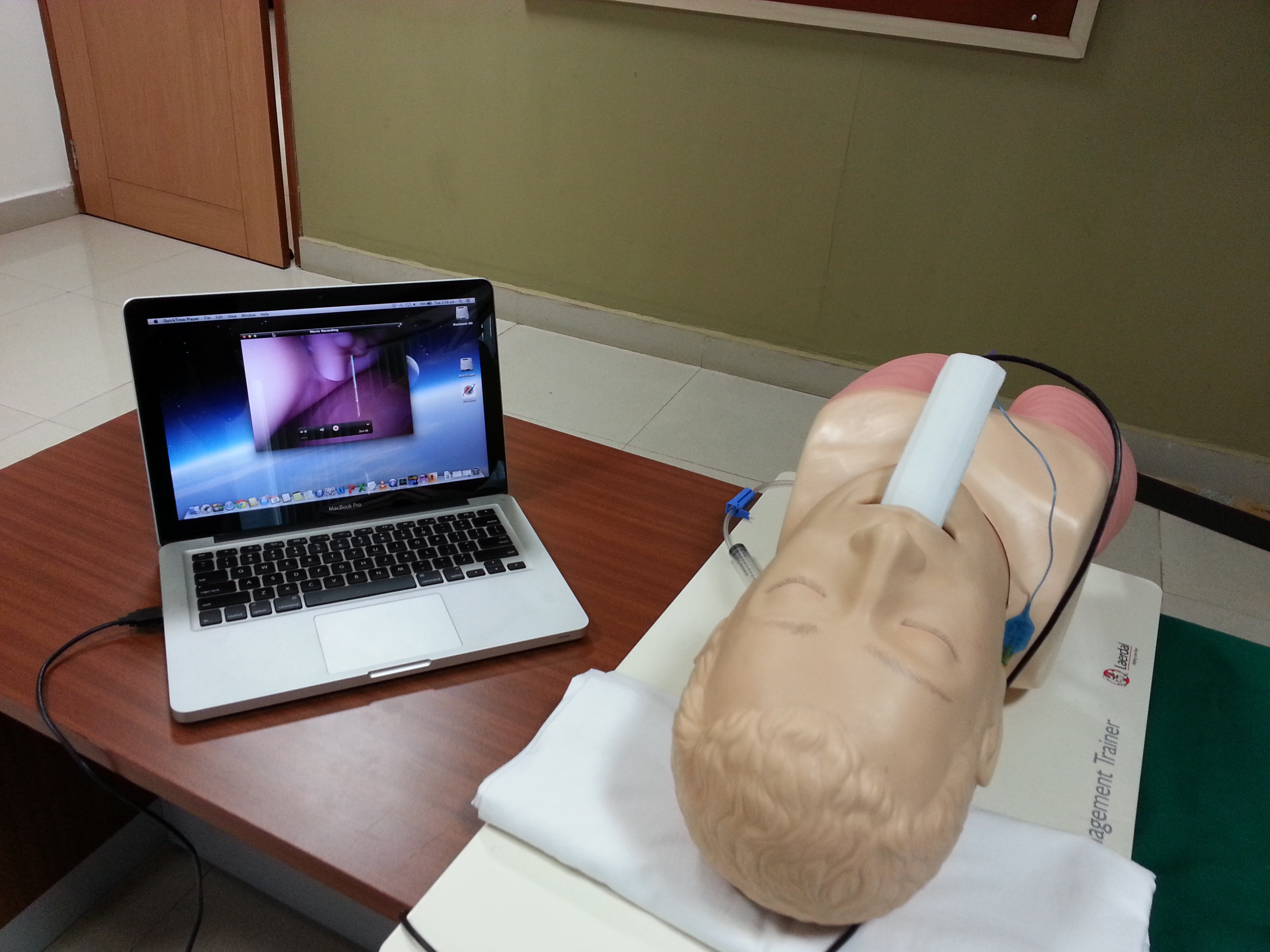
Interestingly, Google Nexus (2012 edition) has inbuilt kernel UVC modules, but needs custom-made software to view the data from the USB device, as the OS doesn’t recognize it as an external camera. The open source Java programming language project called “Simple Webcam” was modified for this purpose ( link here and here) . Videolaryngoscopy and image capture was successful using its large 7-inch color display (Figure 3).
Figure 3

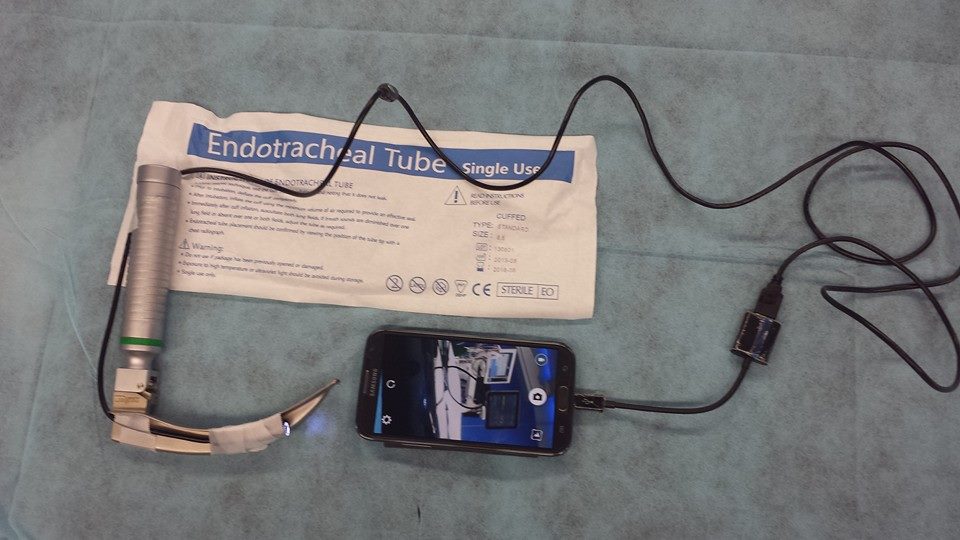
Attempts at reproducing this in other commercial devices like Samsung Galaxy series of mobile phones was initially unsuccessful due to lack of drivers. Technically though, it is possible to convert the data streaming from the micro-USB port to a video stream using custom made software. An application “CameraFi” available through the Google Play App store, created by the Korean company Vault Micro, uses this concept to work on a broad range of devices . The real time video recorded using this application was also of sufficiently high quality for videolaryngoscopy, in a manikin, using an Android phone (Figure 4).
Figure 4
The author also worked on 3D printed prototypes to house the USB endoscope camera that can be used without the need for a conventional laryngoscope (Figure 5). Future efforts would involve, developing further, such open source, low cost commercial videolaryngoscopes that satisfy all regulatory standards, at a large scale. These inexpensive devices could then be deployed in ambulances, emergency rooms, in several critical services in hospitals, especially in developing countries, empowering a wide range of healthcare providers.
Figure 5
(Article was peer reviewed by Dr Reuben Strayer and Dr Seth Trueger)

Reblogged this on MEDEST and commented:
Low budget (but perfectly working) video laryngoscope make us re-thinking about the usefulness of allocating resources in medical equipment. Is there a reason for medical technology to be so expensive? Thanks to the authors every medical professional can understand what there’s behind big companies manufactured devices. It’s time to open our mind and realazing that economical interests (and relaite conflicts) are not limited to big pharma but spreaded in many fields of medical supplies.
My thoughts are that this is a great thing to try in the cadaver lab and in mannequin practice and great to get more experience with rarely available $$$ VL and use for teaching however I have questions about using this clinically.
Are there regulatory approvals or requirements for disinfection in human use? Reusable airway equipment as far as I know has very strict protocols on how they are cleaned and high level disinfected/sterilized and are specific to a particular piece of equipment. Does the material of the equipment and the design of it (e.g. if there are crevices and notches and hard to get to spots, is it completely seal proof after how many uses and after high level disinfection?) impact the ability to clean and disinfect it?
The alternative around those issues is to use stock medical videoscopes or malleable video stylets for that purpose of attaching to regular DL blades but they are also pretty expensive.
Thanks for sharing your experience with this. I am fascinated by this.
Great work guys – always good to see someone trying to cut the cost of of modern healthcare…but I would echo Yen’s concerns about using these devices anywhere other than in manikins or the cadaver lab. There are inexpensive devices available such as the Airtraq (as mentioned above) and the King Vision which is $1000 up front then $15 per blade….otherwise a single use aScope can be taped to a DL blade, but really this is fiddly and not easily done in a hurry. Other videoscopes are expensive because they are precision made and robust, in the case of reusable metal blades they get autoclaved many hundreds of times, in the case of single use blades the camera needs to be robust as it is being inserted into one plastic blade after the next….
If the future lies in disposable blades (with which there are problems – Storz are recalling plastic C-MAC blades in Australia, and I know a few people who have snapped plastic laryngoscopes) we need to get to the stage where they are as reliable as metal blades. If you were going to re-use a home-made device I would want to be very sure that it could be cleaned in a satisfactory way so that you are not going to pass on my prion disease to others (I grew up in the UK during the Mad Cow disease era)!
Having said all that, this kind of initiative might challenge the companies to find cheaper ways to deliver quality products… so power to it.
http://www.ccam.net.au
Medical devices are expensive because there is significant cost in development. All the items shown in your photos represent TENS OF MILLIONS of dollars in development cost. To bring even a traditional DL laryngoscope to market today would cost high 6 figures. And you can’t simply take two currently available products (a borescope and an android tablet) and slap them together and use them on a patient because the FDA says you can’t. There are requirements and standards that have to met and tested to and all of that cost money too. Finally, you need infrastructure and manpower to commercialize a product. While it is true that the actual cost of the parts that go into a product may be small, that is only a tiny part of what goes in to bringing a product to market.
That money has to be recouped and the medical device market is much, much smaller than the consumer market. There are only 100,000 install points for video laryngoscopes in the US if you add up all the ambulances, ER’s and OR’s. We are a long ways away from seeing VL in every crash cart. Since the market size is smaller, the price has to be higher so that a company can actually make money.